 Botany Botany
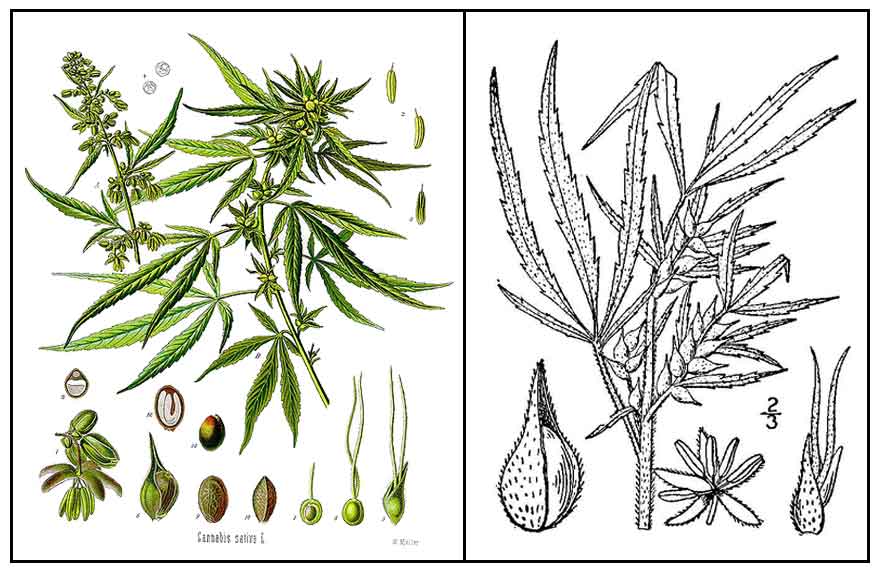
Cannabis sativa is an annual, dioecious, flowering herb. Leaves are palmately compound or digitate, with serrate leaflets. First pair of leaves usually have a single leaflet, gradually increasing to a maximum of 13 leaflets per leaf, usually 7 or 9; and at the top of the flowering plant, again diminishing to a single leaflet per leaf. Lower pairs are usually opposite, the upper pairs alternate. Flowers are imperfect, with staminate (male) and pistillate (female) flowers sometimes in the same plant. Seeds are usually achenes.
 Taxonomy Taxonomy
- Various types of Cannabis have been described: (1) plants cultivated for fiber and seed production, low-intoxicant, non-drug, or fiber types. (2) plants cultivated for drug production, high intoxicant, or drug types. (3) escape or wild forms of both types.
- Breeders and cultivators of drug-type Cannabis categorize cultivars into "pure indica," "mostly indica," "indica/sativa," "mostly sativa", or "pure sativa."
Legality info
- Cannabis is illegal to consume, cultivate, or trade in most countries. While still illegal in most countries, some countries have decriminalized possession and/or its cultivation in limited quantities for personal or medical use. In the United States, 16 states and DC have legalized the use of medical marijuana: Alaska, Arizona, California, Colorado, DC, Delaware, Hawaii, Maine, Michigan, Montana, Nevada, New Jersey, New Mexico, Oregon, Rhode Island, Vermont, and Washington.
Distribution
- Certainly introduced.
- Clandestine cultivation in the highlands, especially the Mountain Province.
- Limited personal-use garden cultivation.
- Native of Asia.
- Commercial cultivation in many countries.
Constituents
- Cannabinoids are terpeno-phenolic compounds secreted by glandular trichomes abundant on the floral calyces and bracts of the female parts. They are responsible for the marijuana "high" one experiences from smoking marijuana.
- Cannabinoids, found only in Cannabis sativa, are secondary metabolites featuring alkylresorcinol and monoterpene moieties in their molecules. More than 60 cannabinoids have been isolated from marijuana or fresh Cannabis leaves.
-
The two cannabinoids usually produced in greatest abundance are cannabidiol (CBD) and/or D9-tetrahydrocannabinol (THC), but only THC is psychoactive. Phenotypes or chemotypes are based on the amount of THC and the ratio of THC to CBD, a ratio that is genetically determined and fixed throughout the life of the plant.
- THC (tetrahydrocannabinol) is the primary psychoactive cannabinoid found in marijuana. CBD (cannabidiol), found in high concentrations in marijuana, is not psychoactive; it has antagonistic effect on cannabinoid receptors and appear to block some of the THC effects. CBN (cannabinol), a major metabolite found in very small quantities in marijuana, is a relatively weak psychoactive cannabinoid.
(29)
- While the marijuana plant contains more than 50 other cannabinoid, the synthetic medications approved by the USFDA (dronabinol and nabilone) contain only THC without CBD. The pharmacologic effects may differ from natural cannabis. (29)
-
Non-drug plants are low in THC and high in CBD, while drug plants are high in THC.
- The drug is derived as dried flower buds (marijuana), resin (hashish), or extracts collectively called hashish oil.
| |
Cannabinoids • Compounds with tetrahydrocanabinol (THC)-like structures and/or THC-like pharmacological properties. Many compounds with THC-like structures are present in cannabis, but not all of them have THC-like pharmacological properties. Some natural or synthetic compounds have THC-like pharmacological properties but not THC-like structure. |
| |
Cannabinoids, the active components of C sativa and their derivatives act my mimicking endogenous substances, the endocannabinoids, that activate specific cannabinoid receptors. They exert palliative effects in patients with cancer and inhibit tumor growth in laboratory animals. |
| |
Cannabimimetic • Tetrahydrocannabinol (THC)-like in pharmacological terms. Four characteristic THC effects in an in vivo assay known as the 'mouse tetrad model" are: hypomotility, hypothermia, analgesia, and a sustained immobility of posture (catalepsy). |
| |
Routes of Administration • (1) Inhaled, the traditional method. (2) As a buccal spray: Sativex, a medicinal cannabis extract containing THC and cannabidiol, administered by spraying into the mouth. (3) Ingested, leaves, seeds, and extracts in various home-made concoctions. Also, as prescribed tablet formulation: dronabinol (Marinol) and nabilone (Cesamet). Other routes of administration, in trials: (4) Intravenous (THC and dexanobinol in saline/ethanol/adjuvant. (5) Rectal (THC-hemisuccinate suppositories (6) Sublingual (THC- cannabidiol-rich cannabis extracts. |
| |
|
Properties
- Cannabis is a popular recreational drug in the world, only behind alcohol, caffeine, and tobacco. In the U.S. it is probably second only to alcohol.
- The psychoactive effects are biphasic: a primary psychoactive effect that includes relaxation and euphoria from its main psychoactive substance, THC. Secondary psychoactive effects include introspection and metacognition. Tertiary effects like increased heart rate and hunger is attributed to 11-hydroxy-THC, a psychoactive metabolite of THC produced in the liver.
- Cannabis sativa cause a "high" commonly associated with hunger (munchies) and energetic feeling while C. indica produces a more "stoned" and meditative feeling, attributed to a higher CBD to THC ratio.
- Reported to have a lower rate of dependence than both nicotine and alcohol, and withdrawal symptoms are typically mild and never life-threatening.
- Considered sedative, stomachic, anodyne, hypnotic, antispasmodic.
- Growing conditions affect potency. Different parts of the plant, like leaves or flower tops, would have different amounts of active chemicals, and therefore, different intoxicant potency. Its variability makes marijuana a crude drug.
- THC is highly hydrophobic. Once absorbed, it binds to lipoproteins and albumin in the plasma and is retained in adipose tissue, its long-term storage site, slowly released back to the blood and other body tissues, with a half-life of 1 to 3 days.
 Cannabinoid Psychoactive Effects Cannabinoid Psychoactive Effects
- Psychoactive effects of cannabinoids in humans is a mixture of depressing and stimulatory effects in the CNS, designated into 4 groups: (1) affective - euphoria and easy laughter (2) sensory - alteration in temporal and spatial perception and disorientation (3) somatic - drowsiness, dizziness, and motor discoordination, and (4) cognitive - confusion, memory lapses and difficulties in concentration.
- Due to the ubiquity of cannabinoid receptors, cannabinoids effects are observed not only in the brain but in almost all peripheral systems, i.e., cardiovascular (fast heart beats), respiratory system (bronchodilation), musculoskeletal (muscle relaxation) and gastrointestinal (decreased motility) systems.
- Cannabinoid effects are variable, sometimes unpredictably strong, with smoked cannabis. In the controlled doses and formulation of dronabinol (Marinol) and nabilone (Cesamet) as antiemetics in patients with cancer, the effect are usually innocuous. Tolerance develops rapidly, psychoactive effects decreasing from 33% to 25% of minor psychoactivity after two weeks, and 4% after 6 weeks of treatment.
- It's addictive potential continues to be debated. Abrupt cessation of chronic cannabis smoking
may occasionally cause a "withdrawal" syndrome, with irritability, insomnia and 'hot flushes." However, this is rare, mild, and usually gone in a few days. Surveys of long-term of use of dronabinol in prescription doses have not shown signs of dependence.
- THC's low addictive potential may be attributed to its pharmacokinetic property - storage of cannabinoids in adipose tissue and low rate of excretion. Cessation of THC use is not accompanied by a rapid decrease in plasma concentration. (•)
Caution
- Already powerful and mind-altering, marijuana is mixed and smoked with other substances, like angel dust (PCP, phencyclidine hydrochloride) or cocaine.
- Marijuana today is much more potent than the 70s. Average THC levels have risen from less than one percent to more than 6% in 2002. Sinsemilla potency has increased in the past two decades from 6% to 13%, with some samples boasting THC levels up to 33%.
- Although the popular myth holds to marijuana's non-addictiveness, current research supports that marijuana is both physically addictive and psychologically addictive.
Delivery routes
- Cannabis is consumed by various routes, most commonly by smoking, followed by vaporization and oral route. Cannabis products can also be taken by ingesting edibles, sublingually or rectal administration, via transdermal delivery, eye drops, and aerosols. (31)
- Use of vaporization for delivery of cannabis to the brain for medical or recreational use has increased. . Heating cannabis at moderate temperatures produces a fine mist of vapors that are inhaled through modified electronic cigarettes, which elicits a similar response without exposure to pyrolytic byproducts. Combustion does not occur; therefore, smoke is not created and saves the user from the over 100 toxins and compounds released from the burning of cannabis. To boot, vaporization reduces the characteristic odor of cannabis smoke, enabling diminished awareness by others. (31) (34)
- Vaping Weed: Vaping is the heating of cannabis without burning. Vaporizers range from cheap and basic models with cartridges full of hash oil to expensive futuristic pods. Among seasoned potheads and occasional users, vaping has become the mode of cannabis use, a lot healthier by many counts for the short-term and long-term risks (cancer) from traditional pot smoking. The vapor is a lot cleaner than smoke from a joint and vapers report less respiratory symptoms. (34)
• Vaping: Bud Vs Oil: Some consider vaporizing the bud as slightly safer than vaporizing the oil. Hash oil may contain adulterants, pesticides among others; some has oil strips THC out of marijuana using lighter fluid or other solvents. For new vapers, caution is advised for strength of the weed. Some hash oil may contain as much as 50%-60% THC, compared to regular weed with 15% to 20% THC. (34)
Parts used
Leaves, stems, seeds, flowers, and oil.
Uses
Edibility / Culinary
- Aficionados and potheads have included marijuana leaves and seeds in a variety of kitchen concoctions: butter, brownies, cookies, salads, and tea, even a vodka drink containing cannabis seeds.
Folkloric
- Cannabis has be used medicinally worldwide for thousands of years.
- Described in ancient Chinese writings, together with ginseng and ephedra, as mainstays of herbal medicine where it was recommended for more than 100 ailments, including gout, rheumatism, malaria, and absentmindedness. Later Chinese texts describe its use for treating vomiting, parasitic infections and hemorrhage. Today, it is still a folk remedy for diarrhea, dysentery and as appetite stimulant.
- In Ayurvedic medicine, used to promote sleep, appetite, digestion, pain relief; also described as aphrodisiac and intoxicant.
- In Africa, used for a variety of ailments, including snakebites, labor pains, malaria, and dysentery.
Others
- Rituals / Religion / Ancient Cultures: (1) Earliest known descriptions of marijuana appear in ancient writings and folklore of India and China, where it was believed to be used as a ritual intoxicant. (2) As early as 2700 BC, carbon-dated reports of cannabis shoots, fruits, and leaves unearthed from Yanghai tombs suggest cannabis was used for ritual/medicinal purposes. (3) Cannabis use is a ritual part of the Hindu festival of Holi. (4) In ancient Germanic culture, Cannabis was associated with the Norse love goddess, Freya. (5) The Rastafari movement embraces the Cannabis as a sacrament.

Studies
• 100 Peer-Reviewed Studies on Marijuana: A summary of 100 peer-reviewed medical studies involving cannabis and cannabis extracts (synthetic products, i.e., Marinol, Nabione, and others were excluded) showed: (1) Double-blind human studies: Total studies, 22; Pro, 12 studies, 54.55% of total; Con, 3 studies, 13.64%, Not clearly pro or con, 7 studies, 31.82%. (2) Human studies: Total studies, 74; Pro 22, 29.73%; Con, 28 studies, 37.84%; NCPorC, 24 studies, 32.43%. (3) Animal studies: Total studies 4, Pro 4, 100%, Con and NCPorCon, 0, 0%. (10)
• Medical Marijuana: A literature review of writings on medical marijuana by 45 researchers concluded established uses for nausea, vomiting, anorexia and weight loss, with "well-confirmed" effect found in the treatment of spasticity, neurogenic pain, asthma, glaucoma and movement disorders, and "less-confirmed" effects for allergies, inflammation, epilepsy, depression, anxiety, dependency and withdrawal.
• Marijuana Policy Project: Clinical trials conducted by the American Marijuana Policy Project have shown the efficacy of cannabis as a treatment for AIDS and cancer patients suffering with clinical depression, and nausea and weight loss associated with chemotherapy or other treatments.
• Cannabinoids / Palliative Effect: The best established palliative effect of cannabinoids in cancer patient is the inhibition of chemotherapy-induced nausea and vomiting. Dronabinol (∆9-tetrahydrocannabinol) and its synthetic analogue nabilone (Cesamet) have been approved for this purpose.
• Synthetic Cannabinoid / Dronabinol: A synthetic version of the cannabinoid THC, dronabinol, may relieve symptoms of anorexia and agitation in elderly Alzheimer's patients. Dronabinol was approved for use in anorexia with HIV/AIDS and chemotherapy-related nausea.
• Glaucoma: Medical marijuana can be used to decrease intraocular pressure of glaucoma. Reduction of intraocular pressure is also achieved with smoking of cannabis, acting on a cannabinoid receptor. However, smoked-cannabis effect is short-lived.
• Analgesic: (1) A single inhalation of 25 mg of 9.4% tetrahydrocannabinol herbal cannabis three times daily reduced the intensity of pain and improved sleep. (2) Study showed THC:CBD extract to be efficacious for relief of pain in patients with advanced cancer not fully relieved by strong opioids.
• Analgesic and Neuro Effects: Medical cannabis is also used for pain relief. It has also been reported beneficial for certain neurologic illnesses such as epilepsy and bipolar disorder. In obsessive-compulsive disorder and Tourette syndrome, study reports a significant decrease in both motor and vocal tics. Study also reports a possible benefit of cannabinoids in preventing Alzheimer's disease.
 • Movement Disorders / Multiple Sclerosis: (1) Smoked cannabis is reported to reduce the spasticity associated with multiple sclerosis. However, the abundance of anecdotal reports are not well-supported by clinical data. (2) In subjects treated with nabiximols (Sativex), as add on therapy, Sativex was shown to improve spasticity in patients who have failed to respond adequately to other antispasticity medications. • Movement Disorders / Multiple Sclerosis: (1) Smoked cannabis is reported to reduce the spasticity associated with multiple sclerosis. However, the abundance of anecdotal reports are not well-supported by clinical data. (2) In subjects treated with nabiximols (Sativex), as add on therapy, Sativex was shown to improve spasticity in patients who have failed to respond adequately to other antispasticity medications.
• Antibacterial Cannabinoids: C. sativa has long been known to contain antibacterial cannabinoids. Study evaluated five major cannabinoids: cannabidiol, cannabichromene, cannabigerol, D9-tetrahydrocannabinol, and cannabinol. All showed potent activity against a variety of methicillin-resistant Staphylococcus aureus (MSRA) strains. (3)
• Short-Term Memory Effect: Marijuana's short-term memory effect occur because THC alters the processing of information by the hippocampus, the brain area responsible for memory function, and where neuron loss accompanies aging and where chronic THC use may hasten the age-related hippocampal neuron loss.
• Lung Damage: Marijuana contains the same cancer causing chemicals found in tobacco. Report suggests that puff-for-puff the amount of tar inhaled and the level of carbon dioxide regardless of THC content are three to five times greater than among tobacco smokers.
• Cannabidiol / Antipsychotic: D9-tetrahydrocannabinol, the main cannabis component, induces anxiety and psychotic-like symptoms in healthy volunteers. These effects are significantly reduced by cannabidiol (CBD), a cannabis constituent that could have anxiolytic and/or antipsychotic actions. Study suggests CBD can be a safe and well-tolerated alternative treatment for schizophrenia. (5)
• Cannabidiol / Antioxidative / Anti-Inflammatory: Cannabidiol (CBD), the isomer of THC, is a potent antioxidative and anti-inflammatory agent to provide neuroprotection in acute and chronic neurodegeneration.
• Degeneration of Alpha Motoneurons / Sciatic Nerve Compression: Study showed the aquatic extract of Cannabis sativa leaves increase the density of alpha motoneurons in spinal cord after sciatic nerve compression in rats. (8)
• Myocardial Infarction Risk in Aging Users: Middle-aged and elderly marijuana users increase their risk of myocardial infarction by more than 4 1/2 times during the first hour after smoking the drug, according to a study presented at the AMA's 40th Annual Conference on Cardiovascular Disease and Prevention. Study also reported an increase in heart rate by about 40 beats per minute, with a rise in supine blood pressure, and an abrupt postural drop, posing a significant risk for people with unrecognized coronary disease.
• Anti-Tumor / Nonmelanoma Skin Cancer: Study reports CB1 and CB2 cannabinoid receptors are expressed in normal epidermis and in skin tumors and that both receptors are functional in the induction of apoptosis of skin tumor cells and the regression of skin carcinomas. Data indicate cannabinoid antitumoral action may also rely on the inhibition of tumor angiogenesis. Study data suggests local cannabinoid administration may constitute an alternative therapeutic approach for the treatment of non-melanoma skin cancer. (16)
• Cognitive Impairment: In a 1996 report of a NIDA-funded study, students who smoke marijuana heavily may be limiting their ability to learn. The study found that college students who used marijuana regularly had impaired skills related to attention, memory, and learning 24 hours after they had last used the drug. (18)
• No Cognitive Impairment: In a 2011 report, an 8-year Australian study of about 2,000 young adults found marijuana has little long-term effect on learning and memory, and any cognitive damage that occurs from cannabis use is reversible. (19)
• Zinc / Reduced Detection: Website claims have been made that zinc sulfate can be an effective adulterant to bypass drug testing. Drug-free urine samples fortified with varying amounts of methamphetamines and benzoylecgonine were tested. Urine samples from acute marijuana smokers were obtained to study the effect of zinc supplements on THC drug testing. Urine drug testing was performed using ELISA detection kits. Results showed both zinc sulfate and zinc supplements are effective in interfering with the detection of all three drugs by Immunalysis drug detection kits. No method was established to detect zinc in the urine samples. Results suggest zinc can be an effective adulterant in urine for some illicit drugs commonly screened on routing drug testing. (20)
• Cannabis Use and Rising Cardiovascular Events: French study reported increasing cardiovascular complications related to cannabis use (with a death rate of 25.6%) indicating cannabis as a possible risk factor for cardiovascular disease in young adults. In a collection of spontaneous reports by the French Addictovigilance Network from 2006 to 2010, 1.8% of all cannabis-related reports (35/1979) were cardiovascular complications, mostly men (85.7%), average age 34.3 years, with 22 cardiac complications (20 acute coronary syndromes), 10 peripheral complications (lower limb or juvenile arteriopathies and Buerger-like diseases) and 3 cerebral complications (acute cerebral angiopathy, transient cortical blindness, and cerebral artery spasm) and in 9 cases, the even led to patient death. Perceived harmless by the general public and legalization of use being debated, the data concerning its danger must be widely disseminated. (23)
• Adverse Outcomes in Long-Term Teen Marihuana Use: Study reports adverse sequelae of adolescent cannabis use are wide ranging and extend into young adulthood. Daily users before the age of 17 had clear reductions in odds of high-school completion and degree attainment, and substantially increased odds of later cannabis dependence, use of other illicit drugs and suicide attempt. (24)
• Potential Benefit of THC in Alzheimer's Diseases / : Study investigated the potential therapeutic effects of Δ9-tetrahydrocannabinol (THC) on slowing or halting the progress of Alzheimer's disease. Results showed THC to be effective at lowering Aß levels in N2a/AßPPswe cells in a dose dependent manner. Low doses of THC can enhance mitochondrial function without inhibition of melatonin's enhancement of mitochondria function. THC can be a potential therapeutic option for Alzheimer's disease through multiple functions and pathways. (25)
• Role of Medical Marijuana in Diabetic Neuropathy: Major cannabinoid, CB1, is expressed in nervous system regions involved with pain perception. Animal models also suggest upregulation of cannabinoid receptors in nerve injury and pain relief with cannabinoides. A randomized, short-term, placebo controlled crossover trial tested the hypothesis that cannabis use can induce dose-dependent reduction in spontaneous and evoked pain with concomitant dose-dependent effect on cognitive function in patients with diabetic neuropathy. Results suggest cannabis can blunt pain of diabetic neuropathy without seriously impairing cognitive function. The higher the dose, the more the pain relief, author Dr. M Wallace said, although there was dose-dependent increase in euphoria. (27)
• Marijuana: The Good and the Bad: The National Academies of Sciences, Engineering and Medicine release a report on the benefits and harms of cannabis use. Among the most significant harms: regular use is associated with mental health risks (psychosis, schizophrenia, social anxiety disorders, suicidal tendencies), respiratory disorders, low birth weight, and increase in motor vehicle accidents. Among the benefits are relief of chronic pain and chemotherapy-induced nausea and vomiting, improvement in spasticity of multiple sclerosis, improve appetite and decrease weight loss in HIV patients, and may improve short-term sleep in MS, chronic pain, fibromyalgia, and obstructive sleep apnea. (30)
• 60 Peer-Reviewed Studies on Medical Marijuana (Cannabis and Cannabis Extracts: 1990-2014): List includes only peer-review studies from 1990 to 2014 on marijuana plant or extracts derived from the plant, such as Sativex and Epidiolex. Studies involing synthetic reproductions, such as Marinol, Nabilone, Cannabinor, and others, were not included. Studies were classified as Pro, Con, Not Clearly Pro or Con. Among some of the Pro studies listed: ALS (Lou Gehrig's Disease), bipolar disorder, cancer (inhibition of breast cancer cell proliferation, benefit for chemotherapy-induced nausea and vomiting), pain relief, decreased spasticity, relief of muscle stiffness, and pain relief in MS patients. For HIV patients, marijuana has shown relief of HIV neuropathic pain, substantial increase in food intake among HIV patients, improved immune function, reduction of PTSD symptoms. Cons include lung problems from regular use, poorer cognitive skills. (32)
• Differentiating Between Hemp and Cannabis: According to a 1976 study published by International Association of Plant Taxonomy, both are varieties of the same genus, Cannabis, and the same species, C. sativa. The difference lies on how the plant is grown and utilized. The term cannabis or marijuana is used to describe the C. sativa plant being bread for its potent trichomes, THC, the cannabinoid most popularly known for its psychoactive properties. Hemp is the C. sativa plant that is bred for industrial uses such as oils and ointments, as well as fiber for clothing, and contains only trace amounts of THC. While Health Canada defines hemp as containing less than 0.3% THC, US law defines hemp as all parts of the C. sativa plant with no psychoactive properties. (37)
Potential Drug Interactions
While data is limited regarding potential drug interactions associated with marijuana use, reactions can be theorized based on metabolism of the primary cannabinoids in marijuana.
•
CYP450 Enzymes: Human have about 60 CYP genes. CYP450 enzymes occur primarily in liver cells where drug metabolism occurs. Chemicals or drugs may be substrates, inhibitors, or inducers of CYP450 enzymes. Substrates are metabolized by the enzyme. Inhibitors reduce the activity of the enzyme, thus preventing metabolism of substrates and increasing substrate concentration and effect. Inducers increase the activity of the enzyme and enhance metabolism of substrates and decrease their concentration and effect. CYP1A2, CYP3A4, CYP2C9, and CYP2C19 enzymes are known to be affected by marijuana use. (1) CYP1A2: Smoking marijuana cause induction of CYP1A2.. This may increase the clearance of theophylline by 48%. Other 1A2 substrates are aminophyline, caffeine, clozapine, estrogens, lidocaine, melatonin, ropinirole, triamterene, zolmitriptan, among others. (2) CYP3A4: The CYP3A4 is involved in the metabolism of both THC and CBD, and 3A4 inhibitors may increase serum concentrations of these cannabinoids. Ketoconazole, a 3A4 inhibitor, can also increase THC concentration by 20&. Strong 3A4 inducers are carbamazepine, phenobarbital, phenytoin, rifabutin, rifampin, St. John's wort, among others. Strong 3A4 inhibitors are clarithromycin, grapefruit juice, itraconazole, ketoconazole, lopinavir, nelfinavir, ritonavir, verapamil, among many others. (3) CYP2C9: In addition to CY3A4, CYP2C9 is another enzyme responsible for the metabolism of THC. Patients who are poor metabolizers of CYP2C9 have threefold higher levels of THC than those with normal 2C9 function. Examples of strong 2C9 inducers are barbiturates, carbamazepine, phenytoin, rifampin, St. John's wort, among others. Strong 2C9 inhibitors are amiodarone, cimetidine, clopidogrel, fluconazole, fluorouraciil, gemfibrozil, valproic acid, among others. (4) CYP2C19: This is another enzyme responsible for the metabolism of CBD. Strong inducers include barbiturates, primidone, St. John's wort. Strong inhibitors include cimetidine clopidogrel, fluconazole, fluoxetine, omeprazole, among others. (29)
ª CNS Depressants: THC can enhance sedative, psychomotor, respiratory and other effects of CNS depressant drugs and alcohol. (29)
• Anticholinergics, Cocaine, Sympathomimetics: Cannabinoids can cause tachycardia. Use of of marijuana with anticholinergics, cocaine, and sympathomimetics can enhance tachycardia and hypertensive effects of cannabinoids. (29)
• Disulfiram and Fluoxetine: Case reports suggest possible interactions of disulfiram (2) and fluoxetine (1) while using marijuana causing symptoms of hypomania. (29)
• Warfarin: A single published report describes a possible interaction with warfarin. The patient, a smoker and regular user of marijuana with multiple comorbidities, taking 10 other medications, had two occasions of bleeding episodes. The only change was an increase in the amount and frequency of marijuana smoking. Author suggests close INR monitoring. (29)
• Antiepileptic Drugs (AEDs): In an open-label safety study of 81 patients with refractory epilepsy, study showed increased doses of CBD showed increase in levels of topiramate,rufinamide, desmethylclobazam, and a decrease in clobazam in both adult and pediatric patients. (29)
Availability
- Wild-crafted.
- Prescription capsules: dronabinol (Marinol) and nabilone (Cesamet).
- Prescription extract, Sativex sublingual spray.
- Seeds in the cybermarket.
|




{kind=link}
{kind=link}
{kind=link}